After the Supreme Court overturned Roe v. Wade in June 2022, the federal government needed a way to protect people seeking emergency care. Especially in states where reproductive health access was changing quickly. I was tasked to lead the design and facilitate new opportunities for people living in America.
One of the strongest tools was EMTALA, the Emergency Medical Treatment and Labor Act. It requires nearly every hospital in the U.S. to do three things in an emergency department:
- Give you a medical screening exam
- Stabilize your emergency condition
- Or transfer you safely if they can’t treat you
While the headlines focused on abortion care, our research revealed something broader: EMTALA protections mattered for many communities. This included people denied care due to race, addiction history, disability, or lack of insurance.
Here are some examples of what EMTALA violations can look like:
- A patient shows up at the emergency room and is turned away because of their race. The hospital does not examine them. That is a violation of EMTALA.
- A patient with a history of opioid use comes in with a medical emergency. The hospital refuses to treat them because of their addiction. That is a violation of EMTALA.
- A hospital sends a patient to another facility, not because they cannot treat the person, but because they do not want to lose money. This is called patient dumping. If the transfer is not safe or medically necessary, it is a violation of EMTALA.
The challenge with these types of laws
There was no clear or public way for patients or providers to report EMTALA violations. The existing complaint system was buried in legacy government tech and only accessible by phone or email. People also had to know exactly how the law applied to their circumstances – and many were afraid to come forward at all, especially in an environment where the very place they were reporting (States, Hospitals) could be the very group that was violating their rights. This caused a significant underreporting of EMTALA violations.
Doing what we could to keep the public safe
I led the design of a public-facing EMTALA complaint portal and educational resources for the public. The first of its kind. It gave anyone in the U.S. a simple, secure way to share what happened in an ER. If the story pointed to a possible EMTALA violation, it would automatically trigger a state-level investigation.
We focused on making the tool and resources:
- Anonymous by default
- Accessible across devices
- Understandable in plain language
Modernizing legacy systems to make it more accessible to everyday people
Behind the scenes, we connected to a backend system called ASPEN, which routes cases to state survey agencies that investigate hospitals. That infrastructure worked, but it was old and had never been made available to the public before.
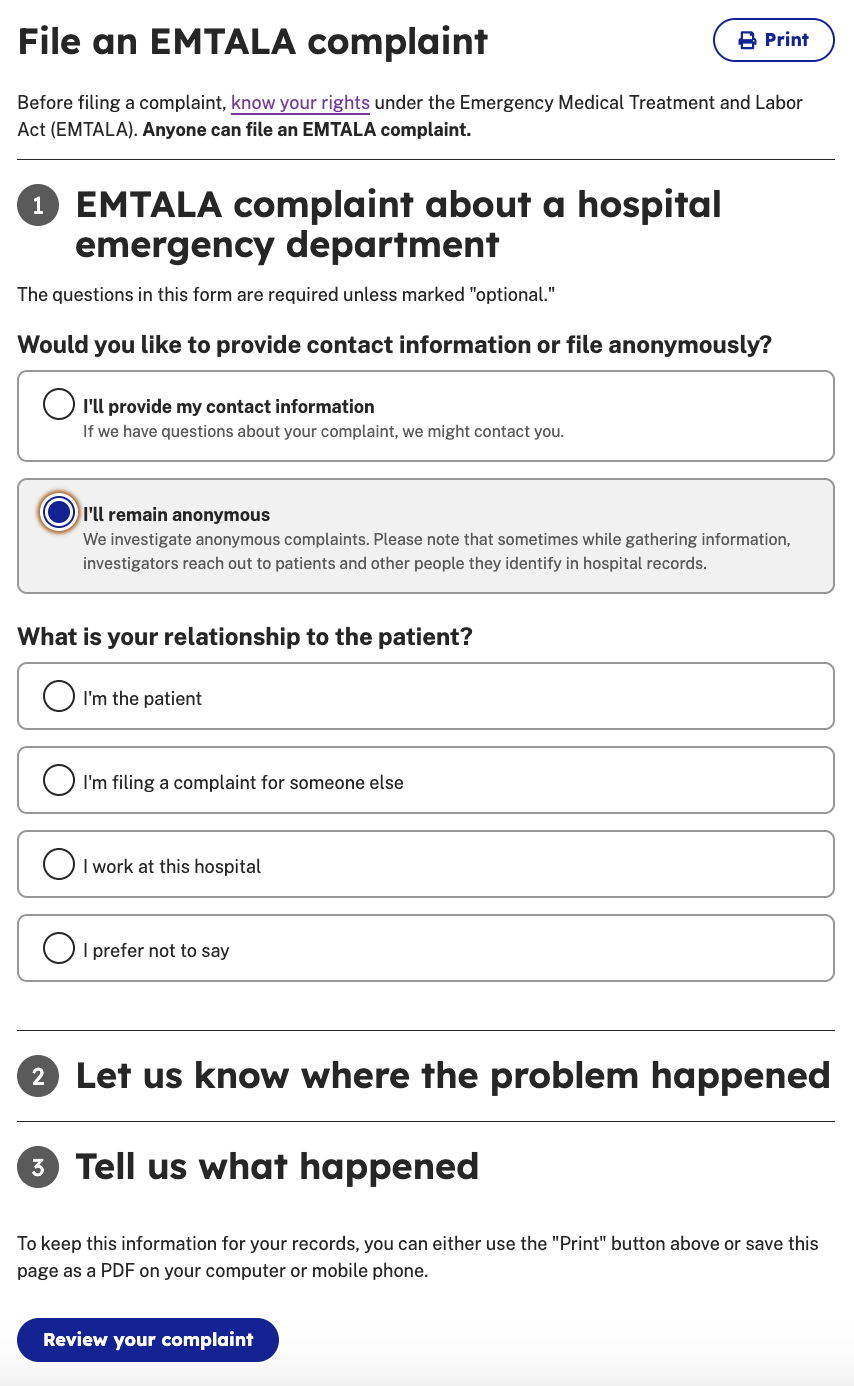
Not very user friendly., but the intake specialists knew it like the back of their hand. To bridge the gap, between specialists and the public I worked across CMS, HHS, and the White House’s Office of Information and Regulatory Affairs to create a trauma-informed, four-question form that avoided government jargon:
- Would you like to provide contact information or file anonymously?
- What is your relationship to the patient?
- Let us know where the problem happened?
- Tell us what happened?
We tested the form with advocacy groups, patients, and frontline organizations to make sure it was easy to use. Because for some people they may be in distress or navigating trauma for one of the worst days of their life. We wanted to make sure that this was as simple as possible… because it truly mattered.
Another goal was that the average person could submit an issue in under 5 minutes. We wanted to reduce the administrative burden as much as possible and shift the burden onto the government.
Impact
This work brought EMTALA protections to life for the public, and not just for lawyers and regulators. It gave patients and providers a real path to report harm, anonymously if needed, and helped federal agencies respond more quickly to civil rights violations in emergency rooms. In the first 5 months of 2024, we saw double the increase of enforcement actions from 2022.
In 2025, EMTALA is still being monitored and updated by the new administration.
Reporting across the web:
- Denied emergency health care? Feds pledge to expedite patient complaints. May 21, 2024 – Washington Post
- CMS Is Making It Easier to Report EMTALA Complaints. Here's What Might Change. – June 19, 2024 MedPageToday